Leucovorin Injection may be given parenterally by intramuscular injection, intravenous injection or intravenous infusion. Leucovorin should not be administered intrathecally.
For intravenous infusion, Leucovorin Injection may be diluted with 0.9% sodium chloride injection or 5% glucose injection before use.
Leucovorin Rescue after High-Dose Methotrexate Therapy: The recommendations for leucovorin rescue are based on a methotrexate dose of 12 to 15 grams/m
2 administered by intravenous infusion over 4 hours (see methotrexate package insert for full prescribing information). Leucovorin rescue at a dose of 15 mg (approximately 10 mg/m
2) every 6 hours for 10 doses starts 24 hours after the beginning of the methotrexate infusion. In the presence of gastrointestinal toxicity, nausea or vomiting, leucovorin should be administered parenterally. Do not administer leucovorin intrathecally.
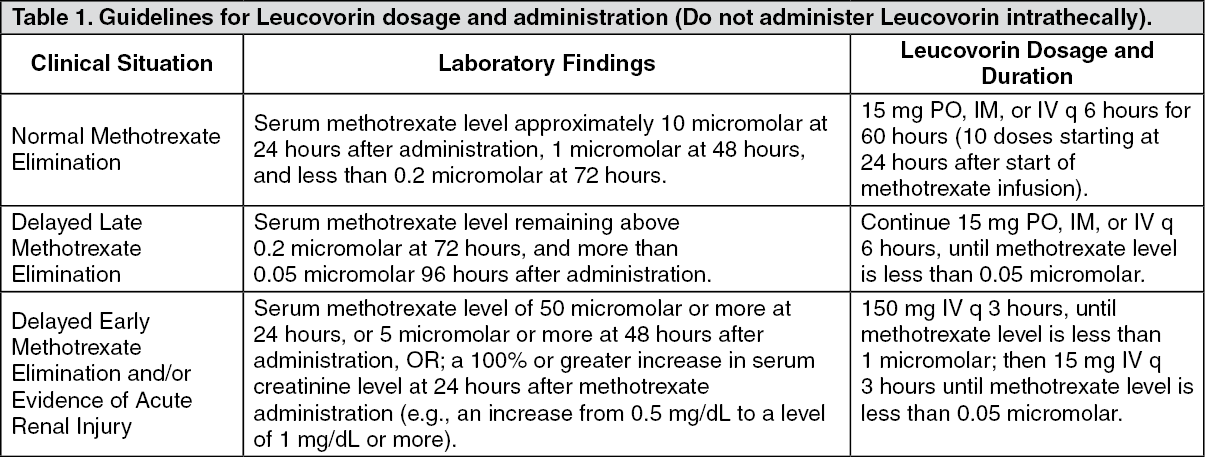
Serum creatinine and methotrexate levels should be determined at least once daily. Leucovorin administration, hydration, and urinary alkalization (pH of 7.0 or greater) should be continued until the methotrexate level is below 5 x 10
-8 M (0.05 micromolar). The leucovorin dose should be adjusted or leucovorin rescue extended based on the following guidelines: See Table 1.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Patients who experience delayed early methotrexate elimination are likely to develop reversible renal failure. In addition to appropriate leucovorin therapy, these patients require continuing hydration and urinary alkalization, and close monitoring of fluid and electrolyte status, until the serum methotrexate level has fallen to below 0.05 micromolar and the renal failure has resolved.
Some patients will have abnormalities in methotrexate elimination or renal function following methotrexate administration, which are significant but less severe than abnormalities described in the table as previously mentioned. These abnormalities may or may not be associated with significant clinical toxicity. If significant clinical toxicity is observed, leucovorin rescue should be extended for an additional 24 hours (total of 14 doses over 84 hours) in subsequent courses of therapy. The possibility that the patient is taking other medications which interact with methotrexate (e.g., medications which may interfere with methotrexate elimination or binding to serum albumin) should always be reconsidered when laboratory abnormalities or clinical toxicities are observed.
Impaired Methotrexate Elimination or Inadvertent Overdosage: Leucovorin rescue should begin as soon as possible after an inadvertent overdosage and within 24 hours of methotrexate administration when there is a delayed excretion. Leucovorin 10 mg/m
2 should be administered IM, IV, or PO every 6 hours until the serum methotrexate level is less than 10
-8 M. In the presence of gastrointestinal toxicity, nausea, or vomiting, leucovorin should be administered parenterally. Do not administer leucovorin intrathecally.
Serum creatinine and methotrexate levels should be determined at 24-hour intervals. If the 24 hour serum creatinine has increased 50% over baseline or if the 24 hour methotrexate level is greater than 5 x 10
-6 M or the 48 hour level is greater than 9 x 10
-7 M, the dose of leucovorin should be increased to 100 mg/m
2 IV every 3 hours until the methotrexate level is less than 10
-8 M.
Hydration (3 L/d) and urinary alkalinization with sodium bicarbonate solution should be employed concomitantly. The bicarbonate dose should be adjusted to maintain the urine pH at 7.0 or greater.
Megaloblastic Anemia due to Folic Acid Deficiency: Up to 1 mg daily. There is no evidence that doses greater than 1 mg/day have greater efficacy than those of 1 mg; additionally, loss of folate in urine becomes roughly logarithmic as the amount administered exceeds 1 mg.
Advanced Colorectal Cancer: Either of the following two regimens is recommended: Leucovorin is administered at 200 mg/m
2 by slow intravenous injection over a minimum of 3 minutes, followed by 5-fluorouracil at 370 mg/m
2 by intravenous injection.
Leucovorin is administered at 20 mg/m
2 by intravenous injection followed by 5-fluorouracil at 425 mg/m
2 by intravenous injection.
5-Fluorouracil and leucovorin should be administered separately to avoid the formation of a precipitate. Treatment is repeated daily for five days. This five-day treatment course may be repeated at 4-week (28-day) intervals, for 2 courses and then repeated at 4 to 5-week (28 to 35 day) intervals provided that the patient has completely recovered from the toxic effects of the prior treatment course.
In subsequent treatment course, the dosage of 5-fluorouracil should be adjusted based on patient tolerance of the prior treatment course. The daily dosage of 5-fluorouracil should be reduced by 20% for patients who experienced moderate hematologic or gastrointestinal toxicity in the prior treatment course, and by 30% for patients who experienced severe toxicity. For patients who experienced no toxicity in the prior treatment course, 5-fluorouracil dosage may be increased by 10%. Leucovorin dosages are not adjusted for toxicity.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image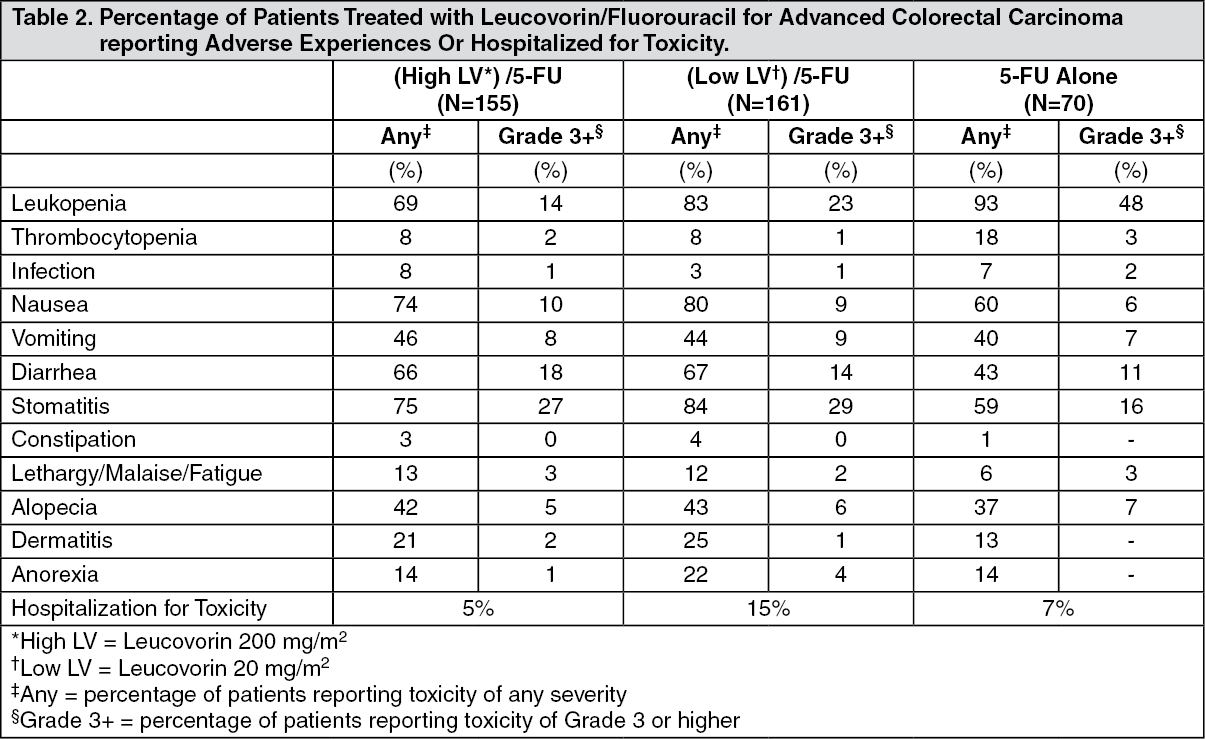 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image



 Sign Out
Sign Out
